NHA Perspective (Speaker: Mr. Himanshu Burad, NHA)
🏛 Galaxy — National NRCeS Adoption & Business Strategy Trends.
ABDM: Moving from Myth to Interoperable Reality
Section titled “ABDM: Moving from Myth to Interoperable Reality”A central theme of Himanshu Burad’s (NHA) perspective is clarifying the fundamental nature of the Ayushman Bharat Digital Mission (ABDM).
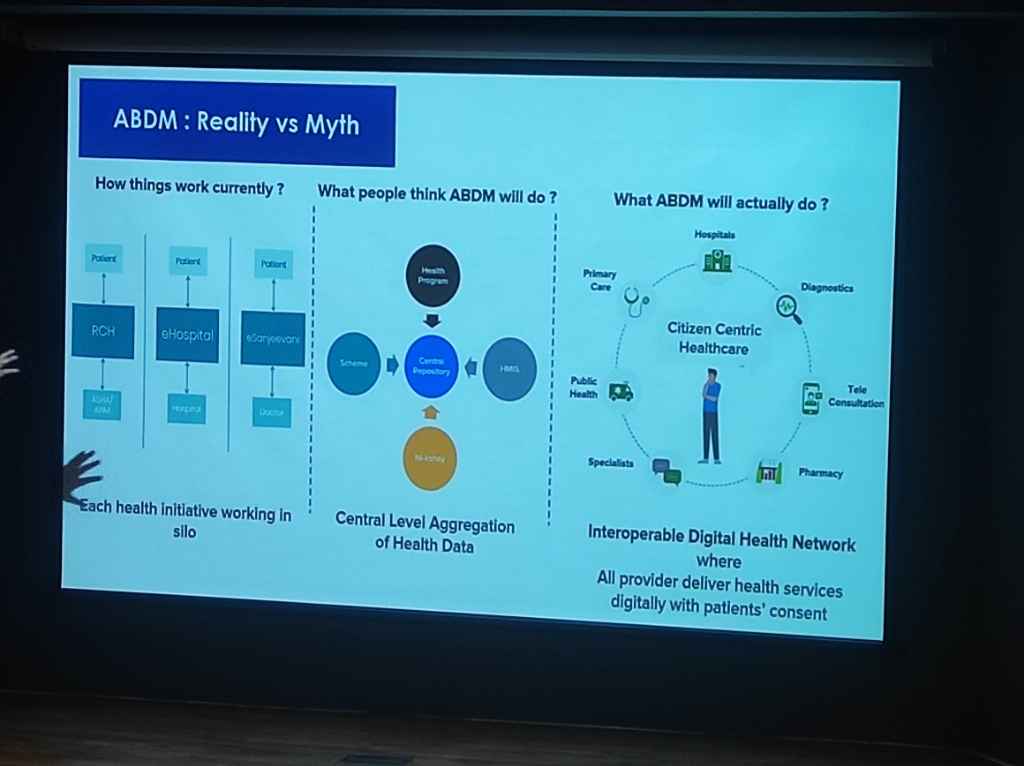 Figure: Shifting from fragmented silos and centralized myths to an interoperable digital health network.
Figure: Shifting from fragmented silos and centralized myths to an interoperable digital health network.
- The Myth: Many believe ABDM is a “Central Repository” where all health data is physically stored in one government server.
- The Reality: ABDM is an Interoperable Digital Health Network. It is a decentralized framework where data remains at the source (Hospitals, Labs, Clinics) but can be exchanged seamlessly and securely with patient consent.
- The Goal: To create a Citizen-Centric Healthcare ecosystem connecting Specialists, Primary Care, Diagnostics, Pharmacies, and Public Health programs into a single, interoperable fabric.
Metrics of Success: Digital Public Infrastructure (DPI) Adoption
Section titled “Metrics of Success: Digital Public Infrastructure (DPI) Adoption”The scale of India’s digital health adoption is now measurable across several core registries and interfaces.
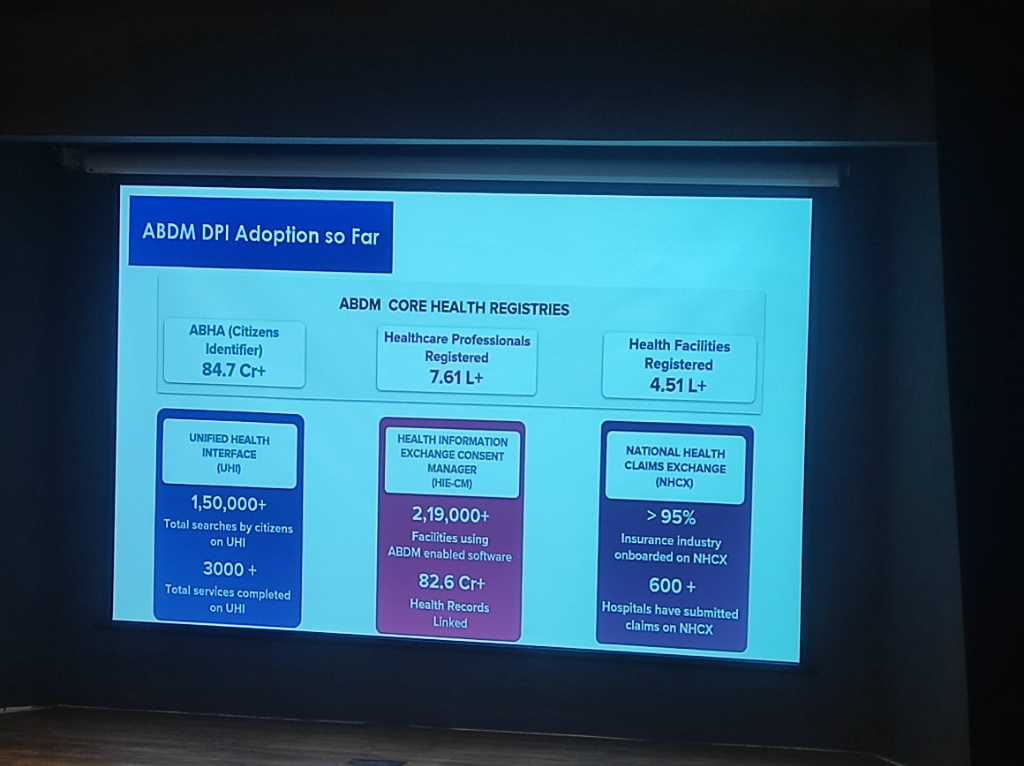 Figure: The latest cumulative adoption stats for ABDM registries and interfaces (as of Jan 2026).
Figure: The latest cumulative adoption stats for ABDM registries and interfaces (as of Jan 2026).
Core Health Registries
Section titled “Core Health Registries”- ABHA (Citizens Identifier): 84.7 Cr+ (847 Million) identities created.
- Healthcare Professionals Registered: 7.61 L+ (761,000).
- Health Facilities Registered: 4.51 L+ (451,000).
Health Information Exchange (HIE-CM)
Section titled “Health Information Exchange (HIE-CM)”- Facility Support: 2,19,000+ facilities are now using ABDM-enabled software.
- Data Linkage: 82.6 Cr+ (826 Million) Health Records have been digitally linked to ABHA IDs.
Impact Platforms: E-Sanjeevani & CoWIN
Section titled “Impact Platforms: E-Sanjeevani & CoWIN”These registries underpin the massive success of national platforms:
- E-Sanjeevani: Over 44.13 Crore consultations completed, averaging 4 Lakh daily.
- Economic Impact: Saves an average of 18 hours and one day’s wages per rural patient.
- CoWIN: Demonstrated global scale by orchestrating a vaccination drive larger than many countries’ total populations.
The ABDM Partner Ecosystem (Speaker: Mr. Himanshu Burad)
Section titled “The ABDM Partner Ecosystem (Speaker: Mr. Himanshu Burad)”A critical role of the national mission is nurturing a diverse ecosystem of partners who integrate with the ABDM to provide a seamless user experience.
 Figure: The diverse ecosystem of ABDM-enabled partners across clinical, insurance, and personal health domains.
Figure: The diverse ecosystem of ABDM-enabled partners across clinical, insurance, and personal health domains.
- PHR Applications: Consumers can use apps like Paytm, Aarogya Setu, eka.care, ninety one, and DRIEFCASE to manage their health records.
- HMIS & LMIS: Hospitals and Labs can adopt ABDM-compliant systems like NextGen, e-Sushrut, Dr Lal PathLabs, and Cloud Pathology.
- Insurance & Pharma: Integrating the entire value chain, including HDFC ERGO, ICICI PRUDENTIAL, Drucare, and SBpirals.
Kickstarting the ABDM Journey (Speaker: Mr. Himanshu Burad)
Section titled “Kickstarting the ABDM Journey (Speaker: Mr. Himanshu Burad)”For clinics and small facilities, the journey toward digital integration is designed to be mobile-first and straightforward.
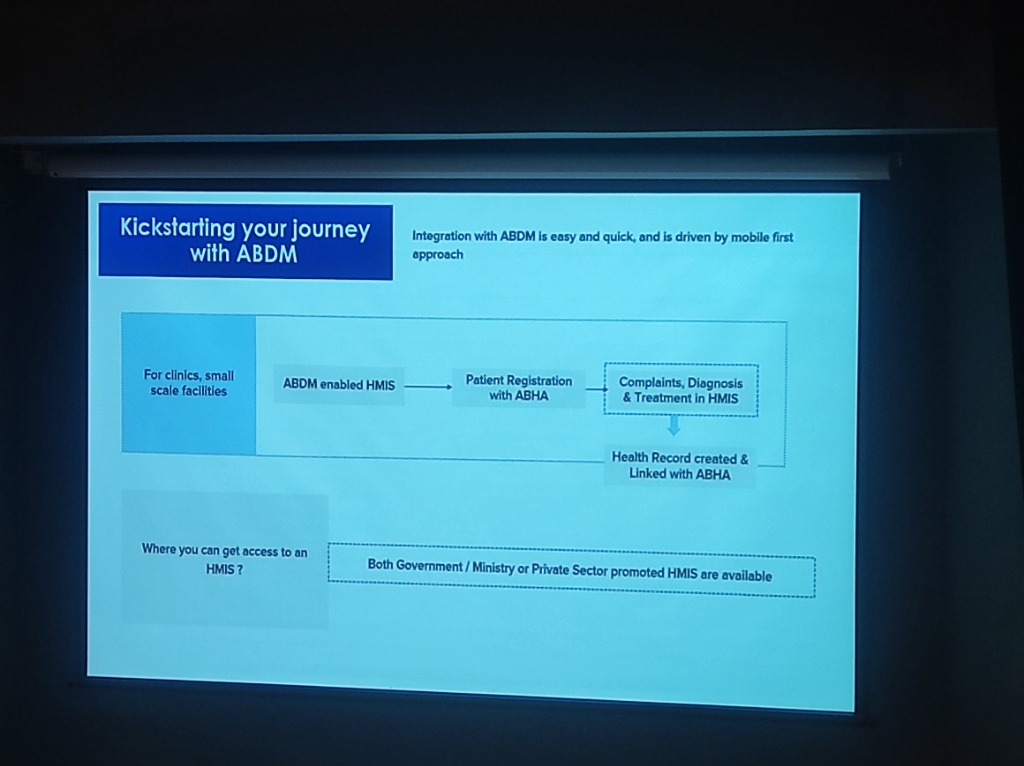 Figure: The streamlined onboarding flow for small healthcare facilities joining the ABDM network.
Figure: The streamlined onboarding flow for small healthcare facilities joining the ABDM network.
- Adopt ABDM-enabled HMIS: Select from a wide list of government or private sector software.
- Patient Registration with ABHA: Digitally verify and register patients securely.
- Structured Care: Document complaints, diagnosis, and treatment within the HMIS to ensure data integrity.
- Link Health Records: Automatically create and link health records to the patient’s ABHA ID for longitudinal access.
Operational Breakthrough: ABHA Scan & Share
Section titled “Operational Breakthrough: ABHA Scan & Share”One of the most tangible wins for patient experience is the Scan & Share functionality using the ABHA QR code.
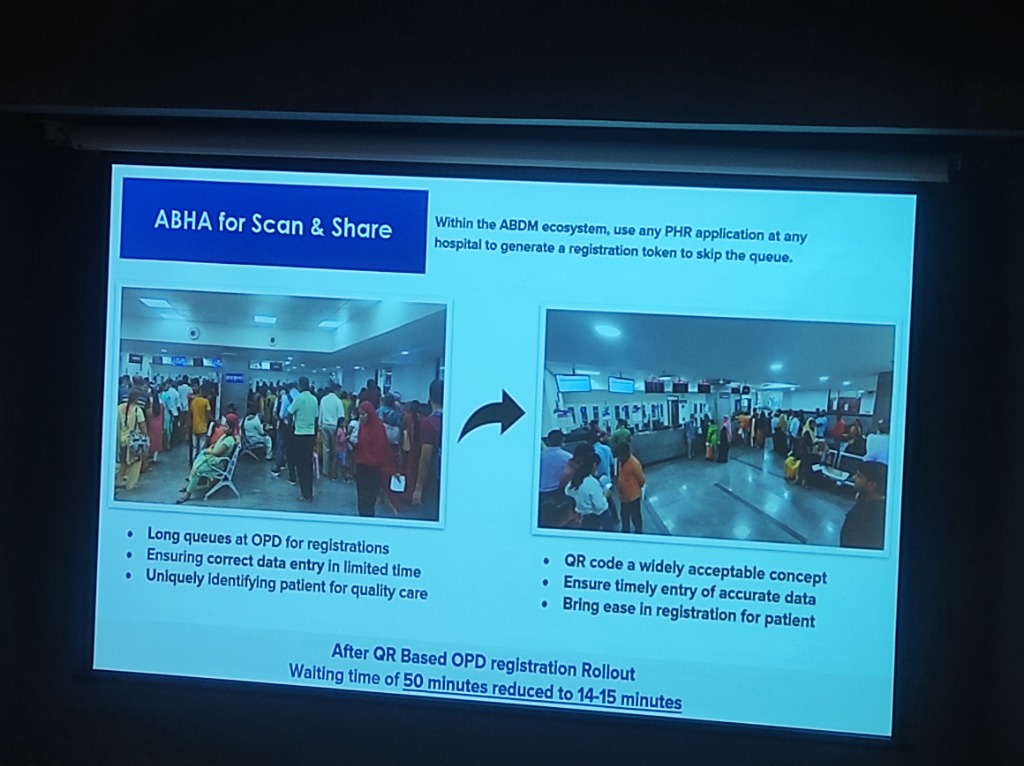 Figure: The impact of QR-based registration on hospital wait times.
Figure: The impact of QR-based registration on hospital wait times.
- The Problem: Long, manual queues at OPD registration desks lead to data entry errors and patient frustration.
- The Solution: Patients use any PHR application (like Aarogya Setu or eka.care) to scan a hospital’s QR code, instantly sharing their demographic profile.
- The Result: Average waiting times have been slashed from 50 minutes to under 15 minutes, ensuring timely and accurate data entry.
Services for Citizen: The Digital Patient Journey
Section titled “Services for Citizen: The Digital Patient Journey”ABDM enables a seamless digital experience for patients, from profile sharing to payment and record access.
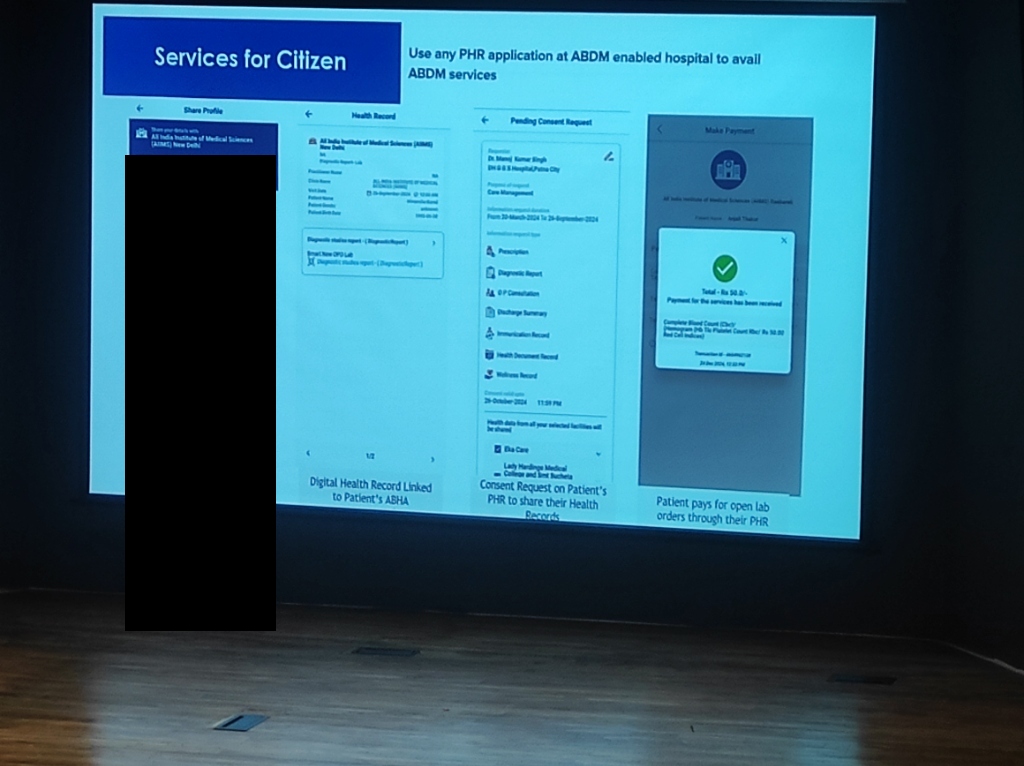 Figure: The end-to-end patient journey: Profile Sharing -> Linked Health Records -> Consent Management -> Mobile Payments.
Figure: The end-to-end patient journey: Profile Sharing -> Linked Health Records -> Consent Management -> Mobile Payments.
- Profile Sharing (Scan & Share): Instantly share demographic info with hospitals to skip registration queues.
- Linked Health Records: Health data from diverse sources linked to a single ABHA ID for longitudinal access.
- Consent Management: Patients grant or revoke access to their health records via mobile-first HIE-CM apps.
- Unified Payments: Seamless payment for lab orders and consultations through the unified health interface.
The Foundation: India’s Internet Journey
Section titled “The Foundation: India’s Internet Journey”The success of these platforms is underpinned by the massive expansion of digital connectivity across the subcontinent.
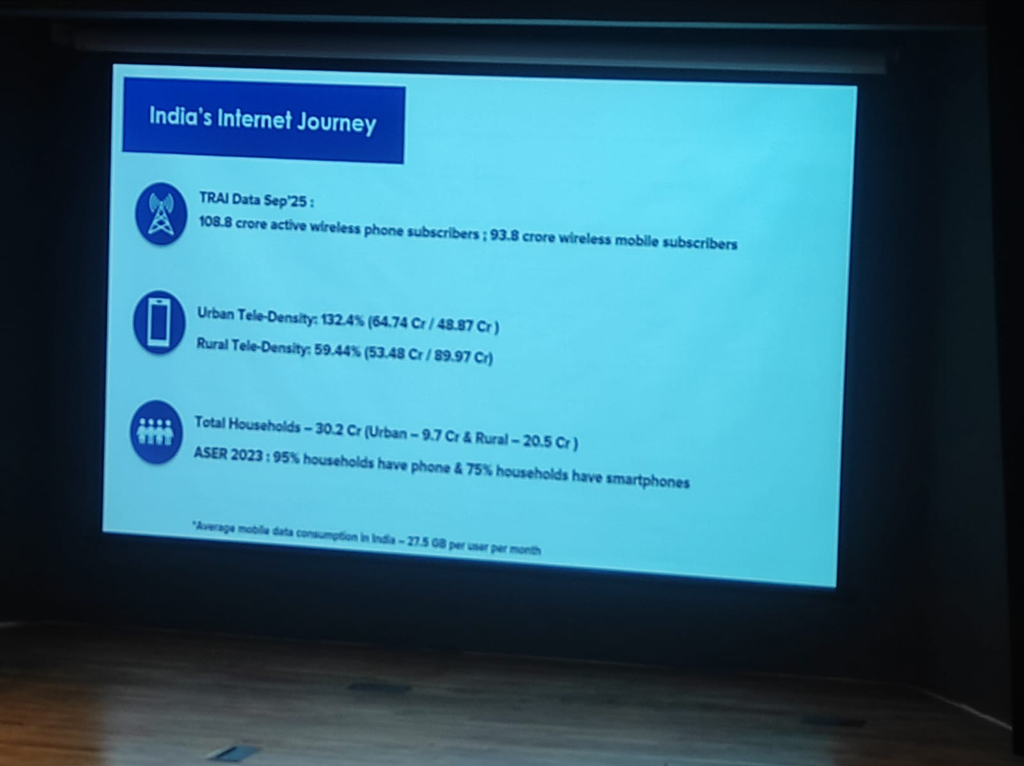 Figure: The growth of mobile and data penetration in India (Source: TRAI/ASER).
Figure: The growth of mobile and data penetration in India (Source: TRAI/ASER).
The Connectivity Boom
Section titled “The Connectivity Boom”As of September 2025, India has 108.8 Crore active wireless phone subscribers, with 93.8 Crore being mobile data users. Average data consumption stands at a global leading 27.5 GB per user per month.
- Rural Coverage: Rural tele-density is at 59.44%, with 75% of households already owning a smartphone.
- Digital Champions: Overcoming digital literacy in rural regions requires empowering local peer-led advocates through modular, hands-on training.
Infrastructure: The Digital Health Highways (Speaker: Mr. Himanshu Burad)
Section titled “Infrastructure: The Digital Health Highways (Speaker: Mr. Himanshu Burad)”The core of ABDM’s strategy is building the “underlying infrastructure” rather than consumer-facing applications. This is conceptualized as the Digital Health Highways.
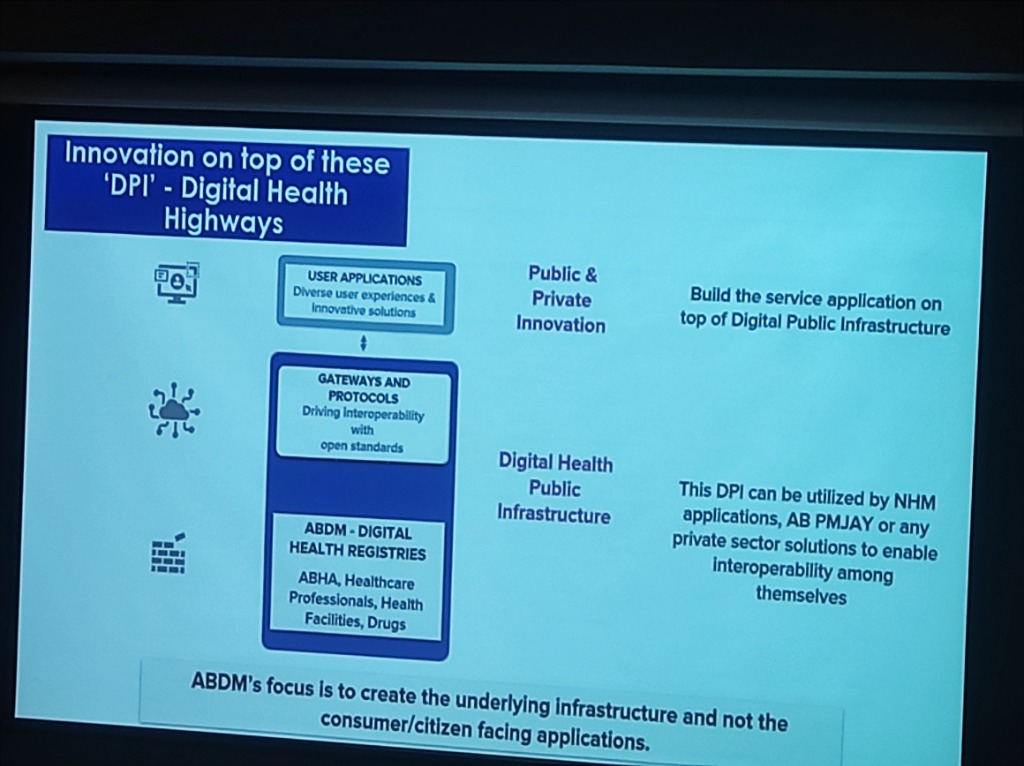 Figure: The layered architecture of Digital Health Highways—from registries to gateways to private/public innovation.
Figure: The layered architecture of Digital Health Highways—from registries to gateways to private/public innovation.
- Layer 1: ABDM Digital Health Registries: The foundation (ABHA, Professionals, Facilities).
- Layer 2: Gateways and Protocols: Driving interoperability with open standards (UHI, HIE-CM).
- Layer 3: User Applications: Providing diverse experiences built on top of the public infrastructure.
The Technical Stack under ABDM
Section titled “The Technical Stack under ABDM”ABDM is designed as a technology stack that enables an open ecosystem based on health data and digital health services.
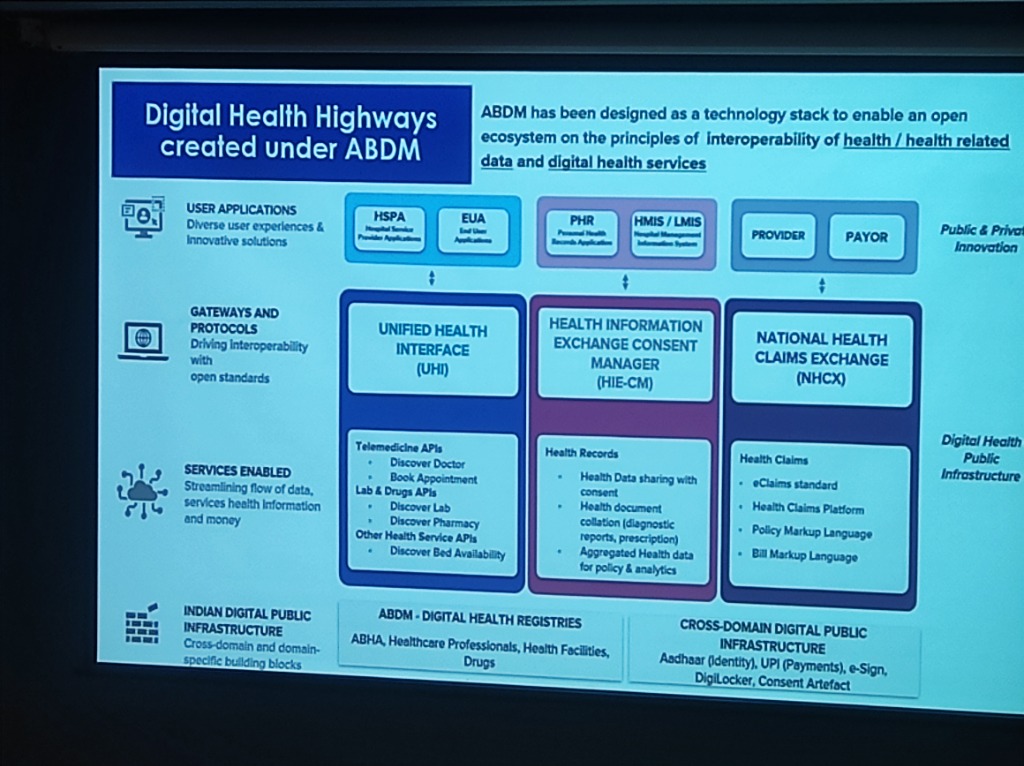 Figure: Detailed architectural view of UHI, HIE-CM, and NHCX as part of the National DPI.
Figure: Detailed architectural view of UHI, HIE-CM, and NHCX as part of the National DPI.
- Unified Health Interface (UHI): For service-level integration (Doctor discovery, appointments, tele-consultation).
- Health Information Exchange (HIE-CM): For longitudinal health record sharing with consent.
- National Health Claims Exchange (NHCX): For automated, paperless insurance claims.
- Cross-Domain DPI: Leveraging Aadhaar (Identity), UPI (Payments), e-Sign, and DigiLocker for a complete digital experience.
Ecosystem Integration: The Interoperability Hub (Speaker: Mr. Himanshu Burad)
Section titled “Ecosystem Integration: The Interoperability Hub (Speaker: Mr. Himanshu Burad)”ABDM acts as the central plug-and-play hub for the entire Indian healthcare ecosystem.
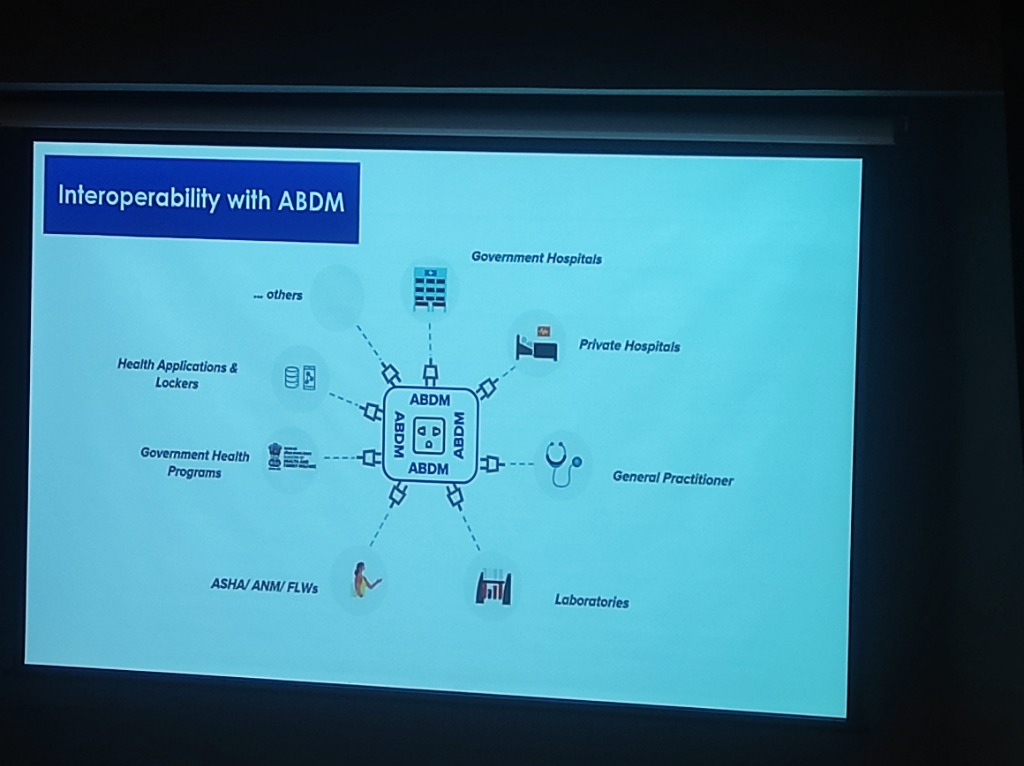 Figure: The ABDM hub connecting government hospitals, private entities, labs, and community workers (ASHA/ANM).
Figure: The ABDM hub connecting government hospitals, private entities, labs, and community workers (ASHA/ANM).
- Seamless Connectivity: Whether it is a large corporate hospital or a rural ASHA worker, ABDM provides the “socket” to plug into the national health network.
- Unified Standards: Ensuring that labs, practitioners, and lockers all “speak” the same semantic and technical language (FHIR/SNOMED CT).
The Strategy: Infrastructure & Governance
Section titled “The Strategy: Infrastructure & Governance”Phygital Delivery Model (Speaker: Dr. Richa Y Singh)
Section titled “Phygital Delivery Model (Speaker: Dr. Richa Y Singh)”The “Phygital” (Physical + Digital) model ensures that technology reaches the “last mile” by integrating community workers (ASHA/Anganwadi) with digital consultation networks.
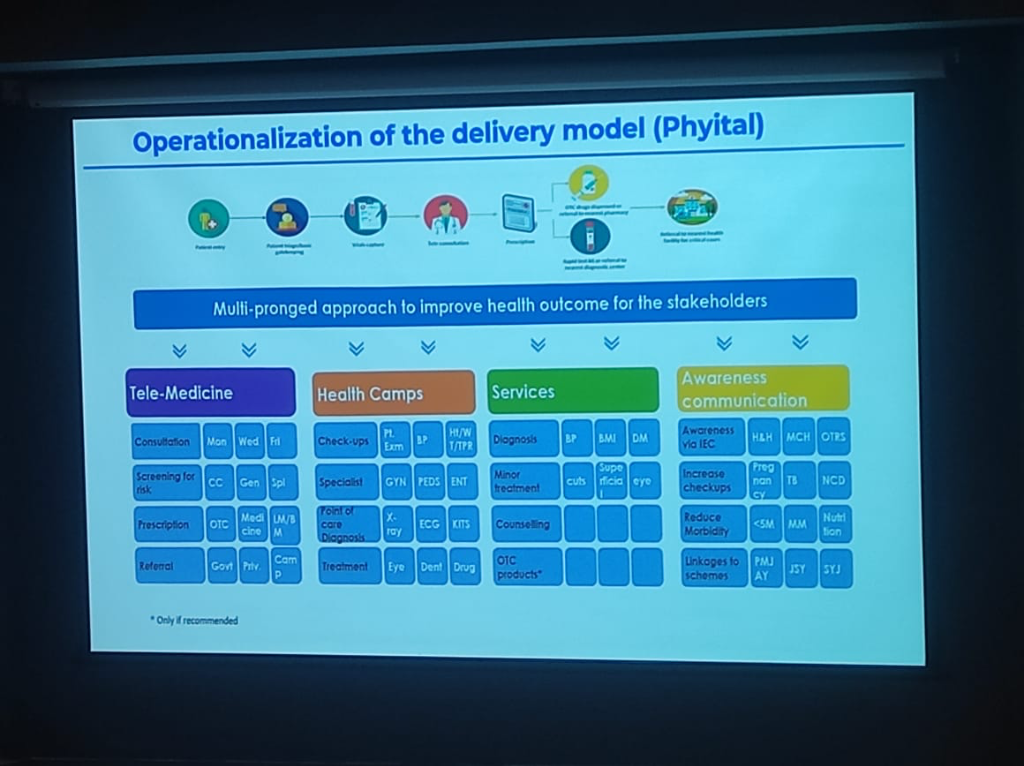 Figure: The Phygital Delivery Model integrating community gates with digital consultation networks.
Figure: The Phygital Delivery Model integrating community gates with digital consultation networks.
NHA’s Role: Auditor of Quality
Section titled “NHA’s Role: Auditor of Quality”The NHA is evolving into an Auditor of Implementation Quality.
- Blind-to-Transit: Privacy-first design ensures NHA has no visibility into health data during transit.
- Institutional Responsibility: The onus of data integrity remains with the clinical source (the hospital).
NHCX: The 30-Second Claim
Section titled “NHCX: The 30-Second Claim”The National Health Claims Exchange (NHCX) is the “UPI for Health Insurance.”
- Current Status: >95% of the insurance industry is already onboarded.
- Efficiency: 600+ Hospitals have submitted automated claims, aiming for a 30-second approval flow by triangulating Identity (ABHA) and Eligibility (via DigiLocker).
Health Data Retention & Private Sector Friction
Section titled “Health Data Retention & Private Sector Friction”The path to universal adoption is paved with both policy mandates and legal complexities.
- Health Data Retention Policy: The NHA has launched a comprehensive Health Data Retention Policy. Any HMIS or health facility integrating with the national backbone must adhere to these standardized retention timelines, ensuring that longitudinal records are not prematurely archived and remain accessible for patient care.
- The Lobby Constraint: Despite the government’s push, private sector participation remains significantly lower. In some states, attempts to mandate ABDM were met with strong opposition from medical lobbies, resulting in court stay orders that have temporarily halted aggressive implementation.
The Strategic Shift: Recognizing these frictions, the national strategy has shifted from “force” or mandatory top-down directives to a model of “facilitation and awareness,” incentivizing adoption through value-added services like NHCX and simplified certification.