Infrastructure Essentials
Infrastructure Essentials: The “Hardware Blind Spot”
Section titled “Infrastructure Essentials: The “Hardware Blind Spot””A critical gap in digital health transformation is the clinician’s awareness of the underlying physical infrastructure. Successful implementation requires understanding the Bill of Materials (BOM) and the foundational requirements for operational stability.
The maturity of a hospital’s digital infrastructure is often determined by its location. The City Classification (Tier 1 vs. Tier 2/3) dictates the “Class of Hardware” available and the feasibility of cloud-native deployments:
- Tier 1 Cities: High bandwidth availability and reliable power make Cloud-Native architectures and advanced hardware deployments more feasible.
- Tier 2/3 Cities: Internet instability often mandates a Heavily On-Premise or hybrid approach, with specialized ruggedized hardware to handle environmental stressors.
On-Premise vs. Cloud-Native: The Strategic Choice (Speaker: Prof. Supten Sarbadhikari)
Section titled “On-Premise vs. Cloud-Native: The Strategic Choice (Speaker: Prof. Supten Sarbadhikari)”| Feature | On-Premise (Traditional) | Cloud-Native (Modern) | Hybrid Approach (Recommended) |
|---|---|---|---|
| Control | Full control over physical hardware and data localization. | Controlled by provider; relies on high-trust SLAs. | Local control for core data; Cloud for elastic services. |
| Infrastructure | Local server rooms with strict HVAC/Fire safety. | Hosted on secure data centers (AWS, Azure, Google). | Tiered: Critical Core on-prem; Scale/Analytics on Cloud. |
| Maintenance | Significant—requires on-site hardware engineers. | Lower—handled by the cloud provider. | Balanced: Internal IT + Managed Cloud Services. |
| Scalability | CapEx-intensive; requires buying new hardware. | Elastic; scales up/down based on demand. | Incremental: Buffer local, burst to Cloud for scale. |
| Connectivity | Fast local LAN; works during internet outages. | Dependent on high-availability internet. | Resilient: Core works offline; Syncs when online. |
| Initial Cost | High upfront investment (Hardware + Setup). | Lower entry cost (Pay-as-you-go). | Moderate: Selective hardware + Subscription OpEx. |
Mission-Critical Design: “Running with Hands Tied”
Section titled “Mission-Critical Design: “Running with Hands Tied””In many clinical settings, direct internet access is prohibited for security reasons. Designing for these “air-gapped” or restricted environments requires a shift in engineering philosophy toward high availability and resilience.
Hospital Network Topology
Section titled “Hospital Network Topology”For a 500-bed hospital, the network must be tiered to ensure that a failure in one ward doesn’t paralyze the entire institution:
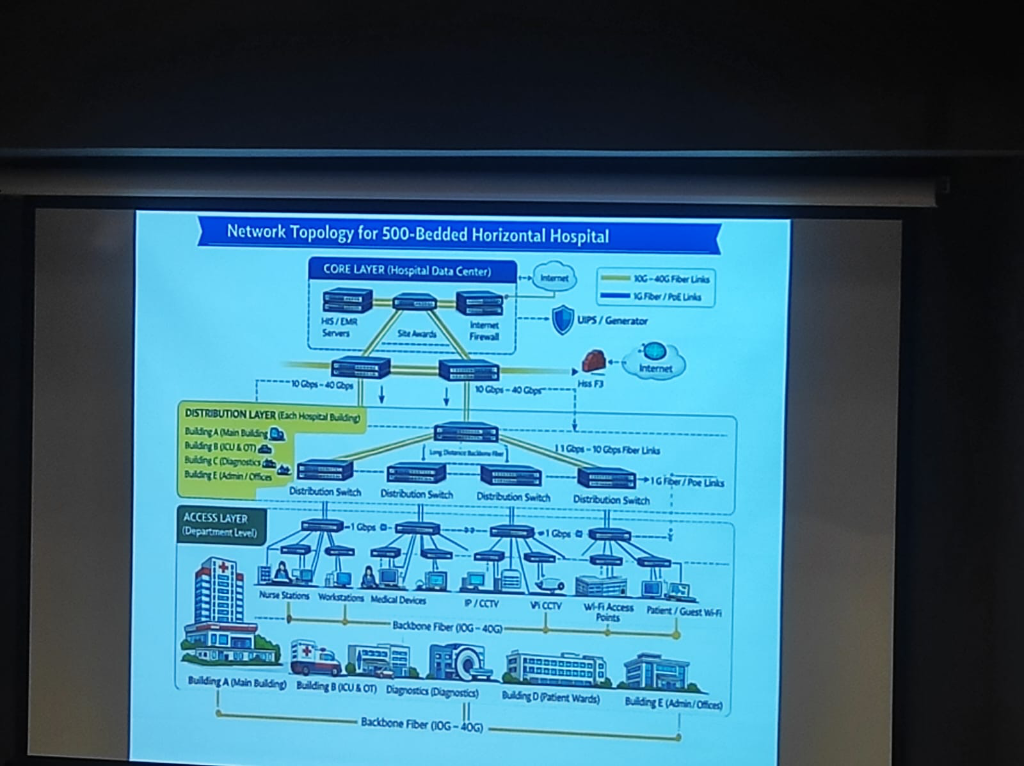 Figure: A formal 3-layer topology (Core, Distribution, Access) designed for zero-downtime clinical operations.
Figure: A formal 3-layer topology (Core, Distribution, Access) designed for zero-downtime clinical operations.
- Advanced Availability Architecture: Hospitals must eliminate single points of failure through a robust technology stack:
- High Availability (HA) & Clustering: Grouping servers into clusters to ensure that if one node fails, another takes over instantly without service interruption.
- Data Replication: Real-time mirroring of clinical databases across multiple storage engines to prevent data loss.
- Failover & Disaster Recovery (DR): Automated failover mechanisms to a secondary Disaster Recovery site (on-prem or cloud backup) ensuring continuity during catastrophic failures.
- Zero-Downtime Resilience: Hospitals cannot afford a “wait period.” Systems must be designed for Triple Redundancy (Local, On-Prem Backup, and DR site) to ensure clinical continuity 24/7.
- PAC Systems & High Throughput: Medical imaging (PACS) generates massive data volumes. This requires High-Throughput Storage and dedicated high-speed VLANs to ensure radiologists and surgeons can access 3D scans instantly without network lag.
- Scalability for Expansion: Infrastructure must be modular, allowing for “plug-and-play” expansion of departments without overhauling the core network backbone.