Wearable Intelligence
The Continuous Monitoring Revolution: Primary vs. Derived Data
Section titled “The Continuous Monitoring Revolution: Primary vs. Derived Data”The integration of wearables marks a shift from periodic snapshots to Continuous Scanning. However, a foundational principle must guide this integration: Medical-grade wearables and consumer-grade devices are not the same.
While consumer ecosystems like Apple Health are prolific, they primarily offer Surrogate or Derived Data, which must be distinguished from Primary Clinical Data:
- Primary Data: Direct, raw clinical measurements or waveforms (e.g., a chest ECG patch providing raw electrical activity).
- Derived & Surrogate Data: Algorithmic outputs that proxy clinical states. For instance, HRV, Heart Rate, and Respiratory Rate on consumer smartwatches are often derived via PPG (photoplethysmogram) sensors and proprietary algorithms.
The Informed Second Opinion
Section titled “The Informed Second Opinion”Managed effectively, consumer data provides a valuable “informed second opinion” for pre-clinical tracking and medication titration, but it carries inherent technical risks:
- False Positives & Alarm Fatigue: Consumer-grade ecosystems frequently generate false positives. Without clinical-grade filtering, these signals can lead to unnecessary patient anxiety and clinician “alarm fatigue.”
- Technical Artifacts: Motion artifacts can significantly distort readings from consumer-grade trackers during daily activity.
- Biochemical Dependencies: Precision varies by technology. For example, Continuous Glucose Monitors (CGMs) use enzymatic reactions (glucose oxidase) that are sensitive to underlying oxygen level fluctuations or respiratory disorders.
- Algorithmic Opacity: Unlike clinical-grade equipment, consumer devices often lack transparent algorithmic validation for their derived parameters.
- Snapshot vs. Continuous Monitoring: A critical void exists in measurement duration. An Apple Watch ECG, for instance, is an on-demand 30-second snapshot—functionally different from hospital-grade continuous telemetry.
- The CGM “Closed-Loop” Gap: While CGM patches provide more frequent data, they are limited by wearable duration (sensor drift after 10-14 days) and, critically, a lack of Closed-Loop integration. In consumer tech, the data is often “monitoring-only,” lacking the integrated therapeutic response required for clinical management.
Wearable Intelligence (Speaker: Prof. Nirmal Punjabi): Extracting Signal from Noise
Section titled “Wearable Intelligence (Speaker: Prof. Nirmal Punjabi): Extracting Signal from Noise”The true “intelligence” of a wearable does not reside in the hardware module but in the Algorithm. This is especially critical because Raw Data is Junk from a clinical perspective, particularly when the user is active.
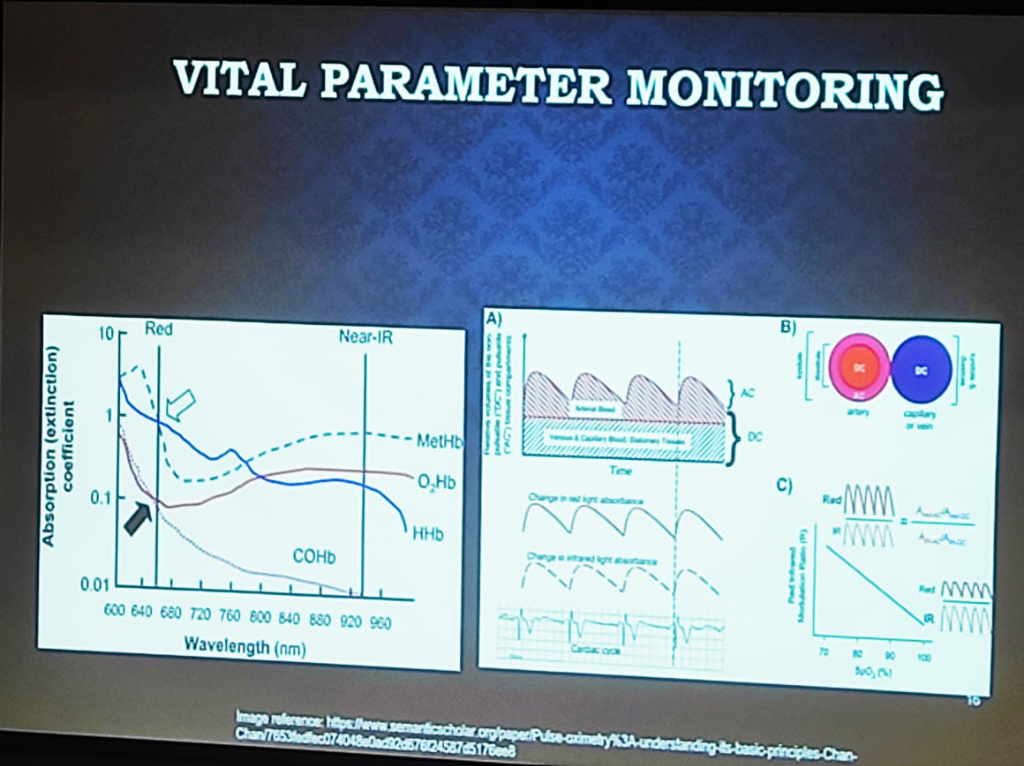 Figure: The physics of Vital Parameter Monitoring—showing the absorption (extinction) coefficients of hemoglobin states and the separation of pulsatile (AC) and stationary (DC) signal components.
Figure: The physics of Vital Parameter Monitoring—showing the absorption (extinction) coefficients of hemoglobin states and the separation of pulsatile (AC) and stationary (DC) signal components.
- The Pulse Oximetry (PPG) Spectrum:
- Medical-Grade: Uses a combination of Red and NIR (Near-Infrared) wavelengths. It relies on the ratio of the pulsatile (AC) part to the stationary (DC) part of the signal across both wavelengths to calculate oxygen saturation accurately.
- Consumer-Grade: Often uses Green Wavelengths (providing maximum reflectance) for heart rate tracking. While these devices handle Single-Point (Snapshot) measurements reasonably well, maintaining clinical significance and signal integrity Longitudinally is a significantly greater engineering hurdle due to baseline drift and sensor-to-skin contact variability.
- Mechanical Interference (The “Tight Wear” Problem): Signal integrity is sensitive to physical application. A common clinical error in consumer wearables is excessive wearing pressure. Wearing a smartwatch or ring too tightly can compress the underlying capillaries and venous structure, distorting the pulsatile (AC) components and altering the stationary (DC) baseline.
- Environmental & Chemical Dependencies:
- Trend over Truth: Most consumer and intermediate-grade CGMs are not designed for spot-check precision. However, in clinical practice, the Trend and Time-in-Range is more than enough for effective monitoring and behavioral intervention.
- The Water Interference Problem: Non-invasive glucose monitoring (e.g., smart rings) faces the challenge of glucose absorption peaks overlapping with water content peaks. Extracting the “glucose signal” from “water noise” remains a significant frontier.
Engineering Actionable Data: Beyond the API
Section titled “Engineering Actionable Data: Beyond the API”Creating an actionable EHR from wearable data requires solving five critical engineering and clinical challenges:
- The Semantic Gap (Algorithm Variance): Identical units (e.g., milliseconds) do not guarantee identical meaning. For instance, Heart Rate Variability (HRV) can be calculated via different formulas—Standard Deviation of NN intervals (SDNN) vs. Root Mean Square of Successive Differences (RMSSD). Different devices generate proprietary “Sleep Scores” or “Stress Scores” that are not semantically comparable.
- The Temporal Gap (Continuance vs. Episodic): Modern EHRs are fundamentally built for Episodic Data—capturing distinct clinical events. In contrast, wearables generate a Continuous High-Frequency Stream. System architects must implement “intermediate refinement” layers that convert continuous streams into meaningful episodic summaries before EHR injection.
- Activity-Aware Normalization: Raw data is meaningless without context. Normalization must be “activity-aware” to create valid Optimal Baselines. Heart rate during sleep vs. heart rate during a activity are two different data points; without normalization, they cannot be used to detect clinical anomalies.
- Contact Verification: Physiological significance relies on signal quality. Modern clinical governance must include algorithms to verify appropriate body contact, ensuring the device hasn’t slipped or lost its sensor-to-skin integrity.
- Clinical Workflow Integration: The final metric of success is the impact on the clinical workflow. Integration must prioritize Burden Reduction for clinicians:
- Event-Based vs. Continuous Flow: Systems should move away from dumping continuous raw datasets. Instead, integration should be Event-Based—where specific algorithmic triggers (e.g., a detection of sustained tachycardia) inject data into the EHR only when clinical attention is warranted.
- Longitudinal Trend Summaries: Clinicians need the ability to view deterioration over time. Rather than relying on proprietary manufacturer scores, institutions should define their own Clinical Indices for trend-based analysis.
- The Actionable Loop (Medication Continuity): Successful models involve trends reviewed to provide active clinical recommendations, including adjustments for Medication Continuity.
- Human-in-the-Loop Escalation: Actionable data must be embedded within an escalation logic, maintaining a “Human-in-the-Loop” for final therapeutic decisions.
- The Practical Delivery Gap (Email/WhatsApp vs. EHR): Most CGM data reports are currently shared via Email or WhatsApp rather than being natively integrated into a professional EHR. True integration requires moving these reports into the core clinical information system.
- Proximity vs. Significance: A foundational clinical principle is that physical proximity does not correlate to physiological significance. A recent example is the Zomato CEO wearing a CGM (Continuous Glucose Monitor); while the device was physically attached and generating data, its physiological significance is limited when used by a healthy individual without clinical indication. Data without clinical intent is merely noise, not medicine.